

This series was supported by the Pulitzer Center.
Part Two in Spotlight PA’s The Cost of Failing series:
The state’s core program to close its psychiatric hospitals and shift care to less-restrictive community programs — the centerpiece of its legal obligation to people with severe mental illness — has instead been used for the past decade to do the opposite, a Spotlight PA investigation has found.
Created more than 30 years ago, the Community Hospital Integration Project Program, or CHIPP, was designed to get people and dollars out of restrictive and expensive state-run psychiatric hospitals and into more effective, community-based care.
The money saved by closing hospital beds would be sent to counties. Former state officials told Spotlight PA the local funds were intended to be sacred — a permanent investment in the care promised not only to the people leaving state hospitals, but to future generations who would need it.
CHIPP was never intended to be the full funder of all things, said Sherry Snyder, a former official in the Office of Mental Health and Substance Abuse Services.
But it was supposed to be “like the mortar between the bricks,” she said.
For a time, the program worked.
But since 2015, the state has stopped closing most vacant hospital beds, abandoning a necessary step toward achieving the program’s public goal of reducing the need for state mental institutions.
Over the same period of time, new funding for community care dramatically slowed.

And in more recent years, the state has spent significantly more money — more than $175 million — on projects to expand psychiatric resources and treatment available primarily for people charged with a crime and in need of specialized care in order to face prosecution.
The spending follows two settlements with the ACLU over unconstitutional wait times for “competency restoration,” treatment for people who cannot understand their legal situation enough to aid in their own defense.
In response to a letter detailing Spotlight PA’s findings, the Department of Human Services said that increased spending on care for people in need of competency restoration is “not a matter of priority — it is a matter of statutory responsibility.”
“[The department] can and does provide recommendations on placement or treatment options when given the opportunity, but it cannot fail to comply with a judge’s order,” said spokesperson Brandon Cwalina in an emailed statement.
The department also emphasizes to county judges and mental health administrators, who are responsible for referring people into state psychiatric care, that such placements should be a last resort, Cwalina said.
A previous investigation by Spotlight PA and the Pittsburgh Institute for Nonprofit Journalism found many of the people referred for this treatment face low-level charges that can stem from experiencing mental health issues in public.
A recent state-backed study supports the newsrooms’ findings. The report found the competency system sweeps up people facing low-level offenses, overrelies on state hospitals to treat them, and leaves them there far longer than necessary.
Because of this, more than one in four patients in a state hospital bed are there because they were charged with a crime, according to a Spotlight PA analysis.
In essence, after a period of psychiatric hospital closures and investment in community support, Pennsylvania has shifted focus to the most restrictive care possible — beds of last resort, for people who have been put at risk in an ill-equipped justice system, for actions that in many cases could have been prevented with care.
When Pennsylvania created the Community Hospital Integration Project Program in 1991, state officials sought to ensure dollars tied to state-run civil psychiatric hospital care remained dedicated to mental health services when that facility closed.
The program shifted the money into grants for county governments, which in turn used that funding to create community-based services beyond what insurance plans cover.
That money, intended to support the people who would have been served by the state hospital, would instead become an annual infusion into the community system.
In the first decade of the program, the state closed three hospitals — Woodville, Somerset and Eastern. A fourth, Haverford, was closed under a different, but similar program. These four closures resulted in a reduction of nearly 1,500 beds. Grants under CHIPP ramped up from $6.5 million to more than $100 million by 2001.
Spurred by patients who sued the state after the landmark Olmstead v. L.C. U.S. Supreme Court decision guaranteed their right to community care, Pennsylvania closed three more hospitals between 2005 and 2011. The move resulted in the discharge of hundreds of patients and the investment of more than $20 million in the community.
Beds closed. Patients rejoined their families and friends. Counties built community resources that gave them a place to live, mental health professionals to keep them on track, and peers with lived experience to provide support.
When the U.S. Justice Department under President Barack Obama’s administration made enforcement of the decision a priority in 2009, state governments created formal “Olmstead plans,” named after the high court decision, to demonstrate how they would move away from institution-based mental health care.
That included Pennsylvania, which drew on decades of success with CHIPP and made the program a key part of its first Olmstead plan.
The 2011 document included firm benchmarks and specific deadlines for the steps necessary to create a community care system. It directed state officials in Pennsylvania’s Office of Mental Health and Substance Abuse Services to request enough funding to shrink the state hospital system by at least 90 beds a year.
The overall goal was ambitious, but simple: “Return all individuals residing in state psychiatric hospital units to their communities.”
That ambition reflected the mood at the time, said Joan Erney, who oversaw the closures of Harrisburg, Mayview, and Allentown State Hospitals as acting deputy secretary of the office from 2003 to 2010. The state was still on a path to close more such hospitals, Erney said, when she left the department.
“We actually had a plan on how we would downsize all of them ultimately,” she said. “And so I think it was hopeful.”
Erney’s successor, Sherry Snyder, signed the Olmstead plan in 2011. At 90 beds a year, this rate would have closed the state’s entire civil psychiatric hospital system over the next two decades.
But Pennsylvania has not closed another state hospital in 14 years.
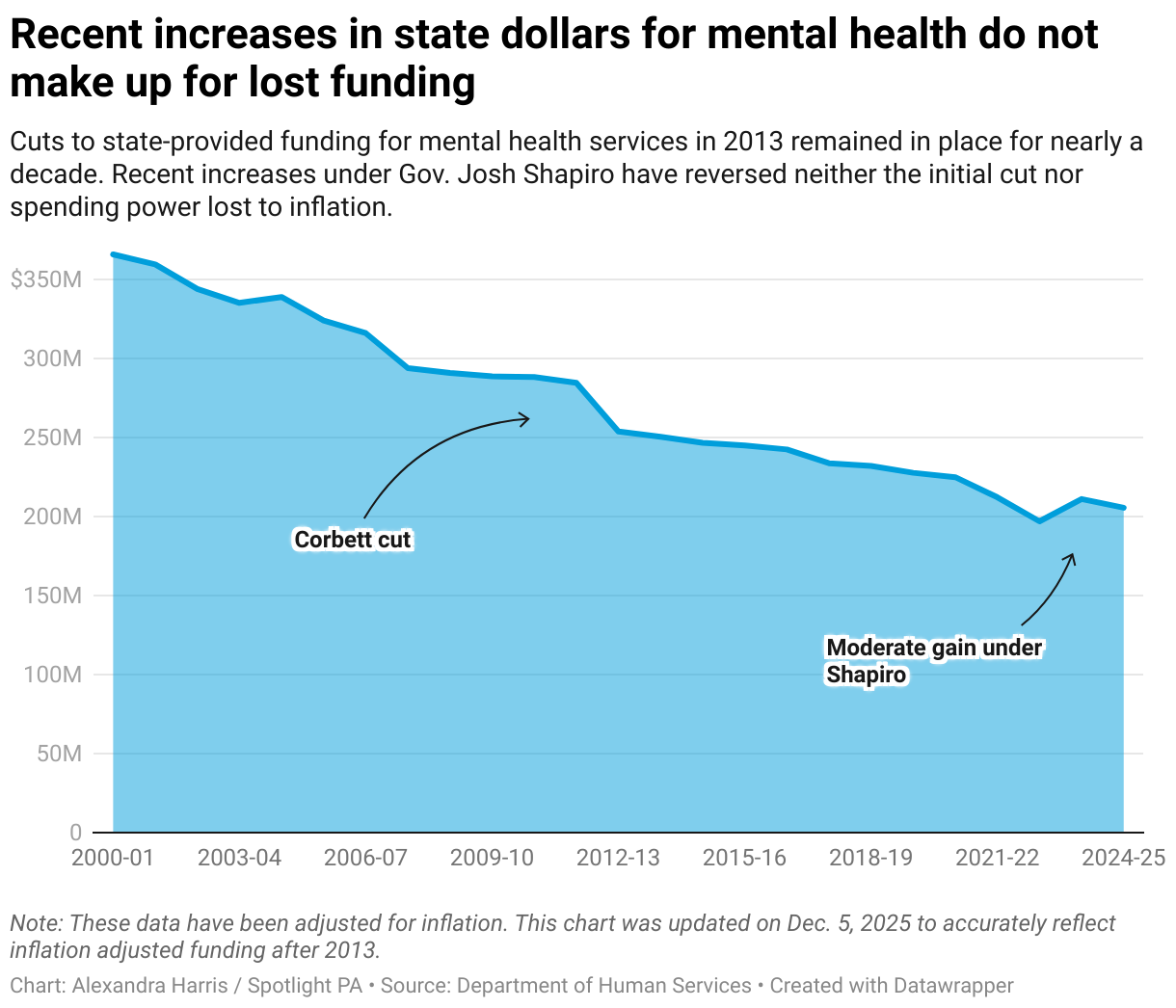
It was February 2012, two weeks after Gov. Tom Corbett announced his budget. In his second year as governor, Corbett took a hard line on spending and proposed deep cuts to mental health programs — including millions from CHIPP.
At a medical assistance advisory committee meeting, government officials, a lobbyist, and a member of the public alike reeled in reaction.
There’s no way services can be maintained, one attendee said, according to minutes from the meeting. The cut is “devastating,” he said.
An audience member asked if the administration was moving away from rebalancing community and institutional care.
Snyder, who worked under Erney and the previous governor, told the committee the cuts would have a deep impact on the department, but the state would hold to its obligation under the Olmstead decision.
The department “will not back away from closing beds,” she told the group.
But privately, she felt the same fears as everyone else.
The final budget cut $44 million from all community mental health spending, which included a roughly $9 million reduction in the CHIPP program.
The cuts “felt like a foundation was falling out,” Snyder said in an interview with Spotlight PA. “I was part of the administration that was trying to build the county base system so people had the opportunity to thrive outside of institutions, outside of jails, in their communities.”
To see that being “dismantled brick by brick, dollar by dollar,” was heartbreaking, Snyder said.
She left the department in late 2012.
But despite efforts to make funding available, Pennsylvania would never hit the goal laid out in its Olmstead plan, leaving the state vulnerable to lawsuits and possible federal action.
While the state more than halved the patient population between 1993 and 2003, the rate of bed closures slowed in the following 20 years. Between 2003 and 2013, the civil patient population decreased by about 42%. Between 2013 and 2023, the civil population fell by about 25%.

Fewer beds closing meant fewer dollars for community resources.
A Spotlight PA analysis found that in its first decade, the CHIPP program grew by more than $100 million. In its second decade, new spending topped $110 million. But in its third, fewer than $40 million in new funding went out to the counties.
The cuts kicked off a vicious cycle: Feeling betrayed, counties became more hesitant to take state dollars, unsure whether they’d be able to rely on the funding, said a former official in the Office of Mental Health and Substance Abuse Services, who requested anonymity to speak more openly about their service.
What’s more, the only way to get those dollars was to give up a state hospital bed, said Tammy Calderone, who has been the mental health administrator for Armstrong and Indiana Counties for 13 years.
After years of closures and consolidation, the patients left in state hospitals were often more complicated and needed higher levels of support in the community than prior groups, county administrators told Spotlight PA. But after the cut, local governments had fewer dollars to cover that more costly care.
Counties were less inclined to give up a state hospital bed to get those dollars, Calderone said. The amount of funding typically provided per patient for closing a bed was about $125,000, Calderone added, which was not enough to meet the substantial care those remaining would need.
“You can't do it for that,” Calderone said.
As counties became harder to persuade to take the money, Department of Human Services officials began requesting less of it in the annual budget despite Pennsylvania’s promises to the federal government.

In 2019, the department under Gov. Tom Wolf requested funding to support only half the state hospital discharges promised under the state Olmstead plan.
The next year, the agency requested fewer: only 20.
When preparing to go before the state legislature and defend her annual budget, former department secretary Teresa Miller would prepare to explain the program’s obvious backslide.
In her role, Miller saw the data that showed the state was not making progress in building community resources, she told Spotlight PA. But in front of the legislature, she would have to defend the state’s position regardless.
“We would go in with a lesser ask and I was always prepared for the, ‘Well, why aren't you asking for the 90?’” she said.
“And the response was, ‘Well, because counties can't spend those dollars.’”
Without the funding, the mortar eroded, and people fell through the cracks.
Counties had less money and fewer hospital beds than ever. Police began arresting a growing number of people with serious mental health issues, a population the state promised to support.
Their behavior was often related to their condition, and in charging them with a crime, the government trapped the most vulnerable people in legal limbo.
Under the U.S. Constitution, if someone cannot aid in their own defense, they cannot stand trial. In Pennsylvania, a judge can order them to receive competency restoration treatment.
This specialized treatment is not primarily intended to help a person recover from mental illness as promised in the Olmstead plan, but to “restore” their competency enough to face prosecution.
For years, Pennsylvania provided that restoration in only two places, Torrance and Norristown State Hospitals. Fewer than 300 beds were available for such care.
People languished in jail for months, waiting for a spot to open. Some waited longer than the maximum sentence for their original charge.
In 2015, the ACLU sued the state.
The class action lawsuit against Pennsylvania argued that by letting these people deteriorate in jail, the state was violating their right to due process under the U.S. Constitution.
The state settled the suit quickly. The Department of Human Services dumped an additional $8 million into community services over the next two years to try to prevent people with mental health needs from landing in jail instead of treatment.
State officials also introduced flexibility into the CHIPP program to rebuild trust with the counties that felt betrayed after the Corbett cuts, said the former official in the Office of Mental Health and Substance Abuse Services. Counties could now, in some cases, accept money from the program without losing access to a state hospital bed.
Between these changes and the settlement, the state created 120 spots for inpatient care in local communities rather than in state hospital beds. More than 375 patients left Norristown and Torrance, according to an ACLU filing.
But it was too little, too late.
After years of declining investment, years of failure to restore cut funding, years of tensions with the counties, the state started reinvesting in mental health care.
To access it, a person just needed to commit a crime.
A year and a half into the settlement with the state, the ACLU found little progress despite the community investment. More people were entering the jails than were leaving. The waitlist for a bed at Torrance or Norristown kept growing.
By 2019, the state responded to the problem by converting about 100 civil beds at Norristown State Hospital to “forensic step-down” beds for people who had recently received competency restoration but still needed court supervision to leave. The expansion has resulted in a 20-year high in the number of people incarcerated in state psychiatric hospitals.
In 2006, about 9% of the patient population across psychiatric state hospitals resided in forensic beds. Today, that share has more than tripled.

This kind of care is not an alternative pathway to treatment, said Jerri Clark, resource and advocacy manager with the Treatment Advocacy Center, a nonprofit that backs civil commitment over criminalization as a solution to broken mental health systems nationwide.
She argued forensic beds are “a punitive system that is restoring some modicum of sanity only for the purposes of further punishing a person,” she said.
Nationally, advocates have seen resources shift toward attempting to “legally adjudicate people for their illnesses, instead of using resources to treat those individuals,” Clark said.
Budget requests lay bare this shift in priorities in Pennsylvania.
Since 2020, the state has invested more than $30 million a year in forensic projects across the commonwealth, while new investment in traditional CHIPP spending has dwindled to under $2 million a year.
Department of Human Services spokesperson Brandon Cwalina said the department encourages counties to invest the forensic grants in programs that could benefit people who are not facing criminal charges, as well as those who are.
But a review of county proposals obtained by Spotlight PA reveals that many are focused on programs for people already entangled in the justice system: competency assessment and restoration programs outside the state hospitals, treatment teams, and long-term residential programs for people with a history of involvement with the justice system.
And in 2022, the state issued a request for proposals to further expand Norristown. It will house 420 people, nearly doubling the size of the forensic system when the ACLU suit was filed.
The project is estimated to cost more than $241 million, nearly the entire size of the CHIPP program.
Coming soon: The struggle to provide care with too many needs and not enough resources.
Correction: A chart in this story has been updated to accurately reflect the inflation adjusted mental health base funding for each year in the data.